

Background and objective. The combination of tyrosine kinase inhibitors (TKI) and chemotherapy (intensive, attenuated or minimal) has improved the prognosis of patients (pts) with Philadelphia chromosome-positive acute lymphoblastic leukemia (Ph+ALL). The combination of HyperCVAD and ponatinib has improved the molecular response and survival compared with other combinations of chemotherapy with first or second generation TKI (Jabbour E, et al, Lancet Haematol. 2018; 5:e618-e627). The Spanish PETHEMA group conducted the phase 2 PONALFIL trial, which incorporates ponatinib to the same induction and consolidation schedule of the ALL Ph08 trial (Ribera JM et al. Cancer 2019;125:2810-2817) The results of this trial after completed recruitment are herein reported.
Patients and method. The PONALFIL trial (NCT02776605) combined ponatinib (30 mg/d) and induction chemotherapy (vincristine, daunorubicin and prednisone) followed by consolidation (high-dose methotrexate, ARA-C, mercaptopurine, etoposide) and allogeneic HSCT. TKI use as maintenance was only scheduled for pts with persistence or reappearance of MRD. By July 2020 the 30 scheduled pts were recruited. The response to therapy (complete morphological [CR], molecular [complete, CMR or major, MMR] after induction and before allogeneic HSCT) (assessed by centralized BCR-ABL/ABL ratio),event-free survival (EFS), overall survival [OS]) and toxicity are herein analyzed.
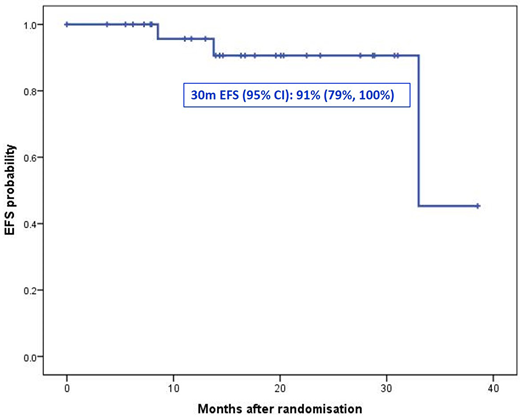
Results. Median age was 50 (20-59) years and 14/30 pts were female. One pt showed CNS involvement at diagnosis. ECOG score at diagnosis was <2 in 86% of pts. Median of WBC count was 6.4 (0.6-359.3) x109/L, Hb 90 (63-145) g/L, platelets 38 (11-206) x109/L. The immunologic phenotype was common in 26 cases, with molecular isoform p190 in 20 patients (67%), p210 in 9 (30%) and p230 in 1 (3%). CR was attained 26/26 patients (100%) (4 are still on induction therapy), with CMR in 11/26 cases (42%), MMR in 6/26 (23%) and no molecular response in 9/26 (35%)).Two patients withdrew the trial (thrombosis of the central retina artery and severe intestinal infection, one case each). Consolidation was given to 24 patients, 2/24 are receiving consolidation and 22 patients received allogeneic HSCT (14 in CMR, 6 in MMR, 2 without molecular response). No relapses before HSCT were detected. No transplant-related mortality was observed to date, but 1 patient withdrew the trial by severe GVHD. Ponatinib was given after HSCT in 4 pts due to loss of molecular response. Three pts relapsed after HSCT, one of them after documented loss of molecular response. All pts are alive (median follow-up of 4.5 months, range 0.5-26.2.2). The EFS probability at 30 months was 91% (79%, 100%) (Figure 1).
One hundred and two adverse events (AE) have been registered in 20 patients, 25 of whom were severe (SAE) and occurred in 14 patients, prompting to withdrawn of the trial in 3 (thrombosis of the central artery of the retina, severe bowel infection, grade IV aGVHD, one case each). The most frequent AE were hematologic (26%), gastrointestinal (15%), infections (10%), hepatic (8%) and cutaneous (5%). Cardiovascular events occurred in 2 patients (angor pectoris and thrombosis of central artery of the retina, one case each).
Conclusions. The preliminary results of the PONALFIL trial after recruitment completed show a high short-term antileukemic efficacy with acceptable toxicity profile.
Supported in part by grant 2017 SGR288 (GRC) Generalitat de Catalunya and "La Caixa" Foundation.
Figure 1. Event free survival (EFS) of the whole series.
Ribera:Pfizer, Amgen, Ariad, Novartis: Consultancy, Speakers Bureau; Pfizer, Amgen: Research Funding. Martinez-Lopez:Incyte: Consultancy, Research Funding; Novartis: Consultancy; BMS: Consultancy, Research Funding; Janssen-cilag: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Janssen: Consultancy, Honoraria. Garcia-Sanz:Amgen: Membership on an entity's Board of Directors or advisory committees; BMS: Honoraria; Gilead: Honoraria, Research Funding; Incyte: Research Funding; Janssen: Honoraria, Research Funding; Novartis: Honoraria; Pharmacyclics: Honoraria; Takeda: Consultancy, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal